
“Mike, forty-one, has shoulder pain which wakes him up at night. Simple movements like pouring water from a kettle would send a jolt of pain down his arm that feels like an electric shock. Now he can’t raise his arm over his head without a pain that makes him grimace and double over.”
The example given in the introduction is a very common example of the debilitating pain that can occur with shoulder muscle trigger-points and strength imbalances between muscles of the shoulder. Although very painful and mimicking a frozen shoulder, excellent results and recovery can be made with manual therapy and rehabilitation exercises.
Anatomy
I think of the shoulder as two joints. Firstly the ball-and-socket connecting the arm (humerus in green) to shoulder blade (scapula). A ligamentous joint capsule encapsulates the ball & socket. The ‘socket’ is very shallow which allows for more movement of the arm, but in turn making it less stable. Over the capsule we evolved 4 ‘Rotator Cuff’ muscles which help hold the ball securely in the socket. So these muscles have to work 24hrs a day, even when asleep.
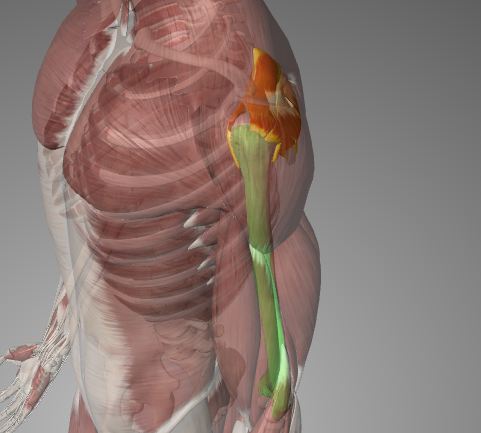
The scapula ‘floats’ on the back of the ribcage, connected purely by muscles. This is named the scapulothoracic joint. The only bone connecting the scapula to the rest of the body is the collar bone (clavicle). It acts as a front ‘spacer’ to help stabilise our shoulder mainly when lifting the arm over your head.
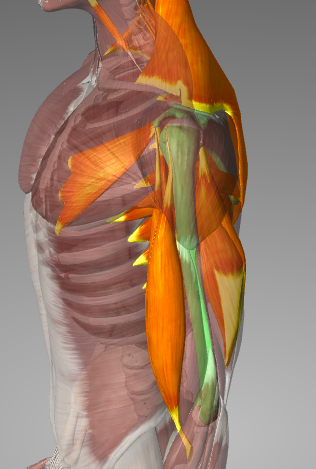
I call all these the foundation muscles of the shoulder joint. In my experience it’s these muscles that can normally cause chronic, non-traumatic shoulder pain. The rotator cuff muscles work 24hrs a day and can be prone to repetitive strain which is commonly caused by long hours at a computer or driving. Strength imbalances are common due to repetitive movement patterns at work or play.
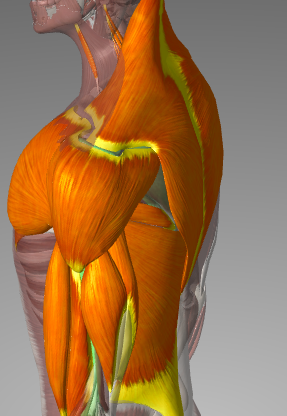
Superficial ‘Power’ muscles
Lastly, there are the shoulder muscles that everyone knows from the gym… Pecs, Lats, Traps, Deltoids, Biceps and Triceps. Bodybuilders tends to focus on these muscles. But if the foundation muscles are weak, compensatory imbalances occur which sooner or later result in pain and/or injury.
The Challenge of Shoulder Pain
Lots and lots of muscles involved in moving the shoulder! There has to be otherwise we wouldn’t have the ability to move our arms in all the ways we can. And we wouldn’t be the humans we are today. The complexity is actually something I enjoy as the challenge is finding which structure(s) is causing shoulder pain before treating. It’s generally more than one muscle causing persistent shoulder pain. And 8/10 the problem is somewhere other than where the pain is!
Do you get pain sitting? At a desk, behind the wheel or even just sat on the sofa trying to relax at end of the day..? Muscle tightness, inflexibility of the ribcage and repetitive strain can all cause pain. The 7 most common issues when sitting at a desk – at what to do about them – are listed here.
A relatively common gissue with regular gym goers with pain is the ‘foundation’ muscles that are relatively weak or over-compensating. Desperately trying to find some ‘scapula stability’. With the elderly or sedentary it’s common for shoulder pain to occur because of deterioration or ‘fixed’ postures. Sometimes periods of overusing the shoulder punctuated with some innocuous sudden ‘jarring’ movement of the arm can cause painful muscle spasms (if not a tears) that stubbornly linger.
Other Causes of Shoulder Pain
Studies have found up to 25% of all adults can experience some shoulder pain at any one time. Bone fractures, major soft tissue injury, joint capsule damage, arthritis, infections or tumours are all local conditions which need referral to a hospital. Also shoulder pain in a very small minority of cases can be referred from more serious conditions – such as strokes, heart disease, liver disease and lung cancer. They can all cause referral pain to the shoulder(s). If worried about any unexplained pain with any other symptoms please consult your doctor.
Manual Therapy, deep tissue massage and myofascial release are effective treatments for muscular shoulder pain, often giving instant relief from pain. A stretching and exercising program to provide a long-lasting resolution to the problem will be given to all our clients. Contact Marlow Sports Therapy to book an appointment and see if we can help you today!

 Enter your name and email and request our free ebook: 7 Habits of Highly Effective Runners
Enter your name and email and request our free ebook: 7 Habits of Highly Effective Runners